
There are simply no contraindications to the use of digital technologies when planning future surgical interventions, and the question of their implementation depends only on the dentist himself. The development of technologies in the field of X-ray diagnostics, as well as an engineering breakthrough in approaches to the production of surgical templates, have significantly expanded the possibilities for planning implantological intervention and subsequent prosthetic restoration of the problem area of the dentition. This outcome was made possible thanks to the combination of several separate disciplines, which provided increased productivity and digital data transfer at different stages of dental treatment.
Revolution or evolution?
Despite the significant breakthrough, many dentists still avoid using computer technologies in their daily practice. The introduction of digital technologies into the work of the clinic requires the adaptation of all working personnel to them, as well as the modification of the workflow as a whole, therefore, all members of the treating team should be ready to learn new skills and techniques in order to keep up with the times, as they say. And innovations continue to appear and develop. Thus, whether the use of digital technologies in dentistry is an evolution or a revolution depends not so much on the technologies themselves as on the individual experience of people who are ready to work with them.
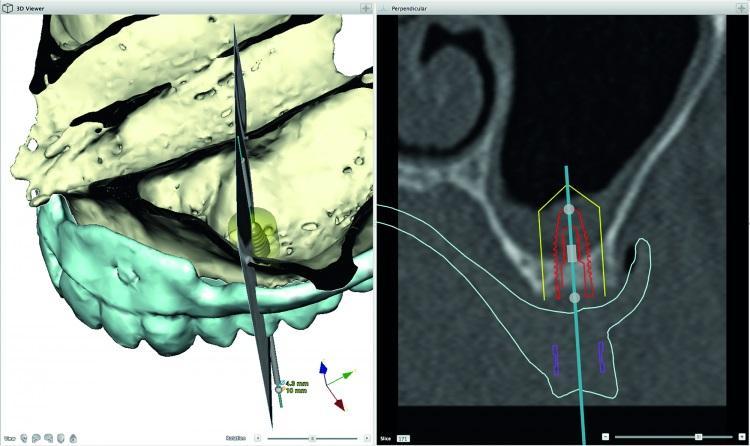
Virtual implantation planning based on computed tomography data helps the doctor and the patient to more objectively approach the choice of the most appropriate treatment method (photo 1). In such cases, the implants are installed with high accuracy, and in the future this ensures a high level of predictability of the surgical and orthopedic stages of treatment. In some particularly difficult clinical situations, doctors can ensure the stability of the achieved rehabilitation by producing an appropriate mouthguard designed according to a stereolithographic model. Also, before starting treatment, you can objectively assess the prospect of performing a completely flap-free operation, as well as the need for certain augmentation interventions. Especially for elderly patients, such a digital approach helps to reduce the time of intervention, as well as minimize the degree of its invasiveness.
Photo 1: Virtual 3-D implantation planning based on tomography data.
In addition, the ability to analyze digital models of the prosthetic bed, as well as the anatomical features of the jaws, contributes to the selection of the most optimal designs based on implants: whether removable or non-removable prostheses. With the help of digital technologies, it is possible to pre-predict the nature of bone resorption in the area of future peri-implant sites, taking into account the possibility and need for appropriate reconstructive manipulations.
CAD/CAM technologies in prosthetics on implants
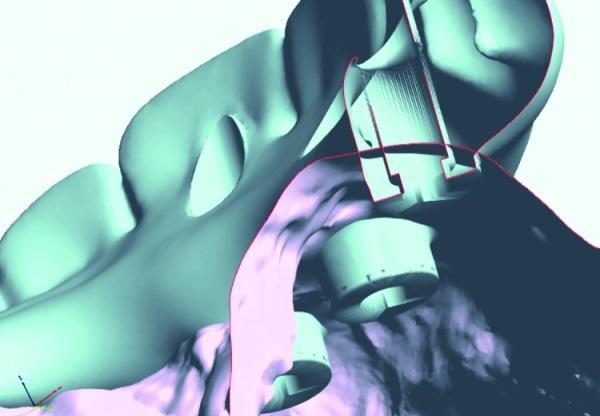
CAD/CAM (Computer-Aided Designing/Computer-Assisted Manufacturing) technologies have significantly changed the development of the dental industry over the past twenty years. The more dental implants can be installed in parallel with each other, the easier and easier it will be to design the frame of the future prosthesis (photo 2) from titanium or zirconium oxide in adapted software. With this approach, biological and technological complications are becoming less and less common. Depending on the type of connection of implantological systems, as well as on the type of all – arc restoration, it is possible to design the connection of elements of infra-and supraconstructions directly at the implant level (photo 3).
Photo 2: Digital CAD / CAM design of the prosthesis frame.
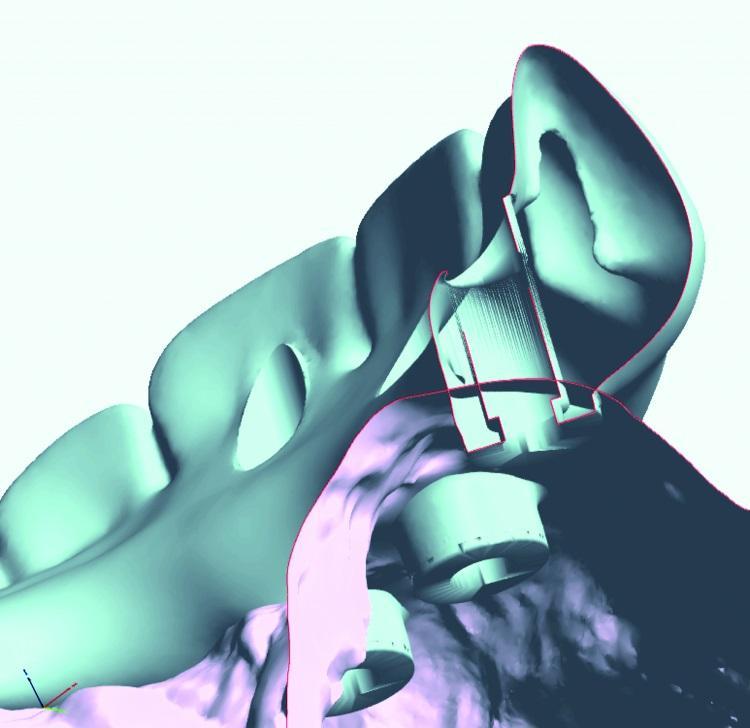
Photo 3: All-ceramic restoration.

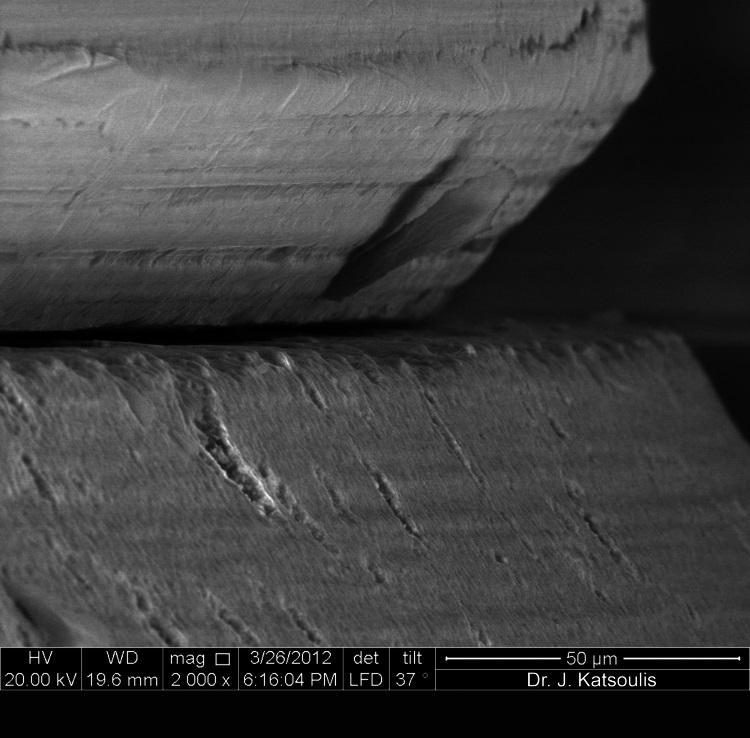
The accuracy of the fit of CAD/CAM-milled titanium or zirconium structures is significantly higher than that of bridge prostheses made by casting. To date, most major manufacturers offer their own CAD/CAM systems and have specialized production centers for mass production of prosthetic frames to order. Thus, CAD / CAM technologies make it possible to achieve a landing accuracy above 50 microns (photos 4 and 5), which is almost impossible to achieve by any other method of manufacturing orthopedic components.
Photo 4: The accuracy of landing is about 50 microns: such compliance can be achieved when using CAD/CAM technologies for the production of all-arc restorations, thus ensuring passive packing of the structure without excessive stress.
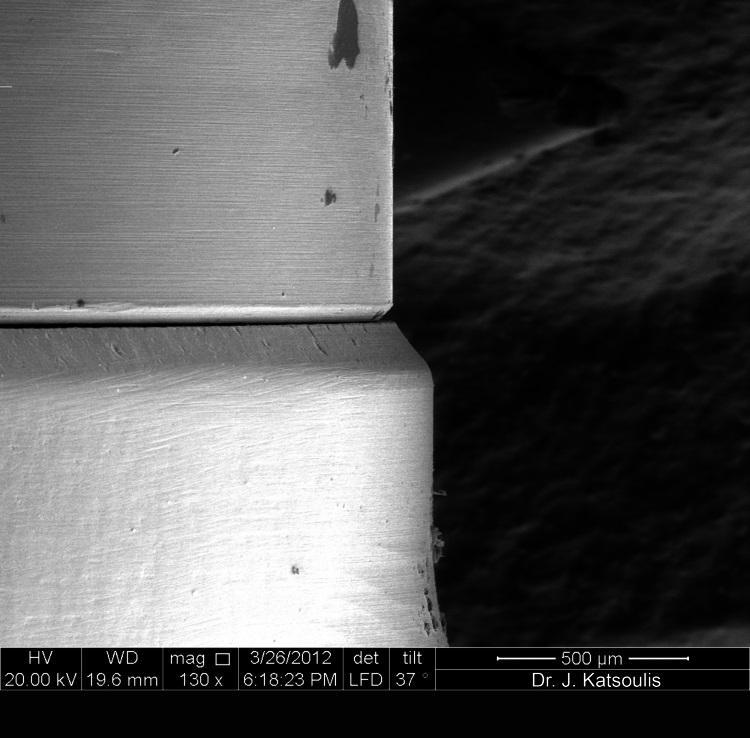
Photo 5: Landing accuracy of about 50 microns: such compliance can be achieved by using CAD/CAM technologies for the production of all-arc restorations, thus ensuring passive packing of the structure without excessive stress.
CAD / CAM production of different materials has its own specific features. During metal milling, special cutting parts are used. After milling of zirconium dioxide, the final crystallization of the part is carried out with a mandatory sintering process, and, despite the automation of almost all production stages, without proper control of experienced engineers, all the achievements of digital technologies can simply be reduced to zero. The aspect of software adaptation also remains the most relevant now: the universal data format (STL) allows you to import scan results into any programs for further analysis and processing. However, it will take some time until various developers make their software completely open so that the doctor can independently choose the appropriate utilities for certain stages of treatment.