Intervention technique
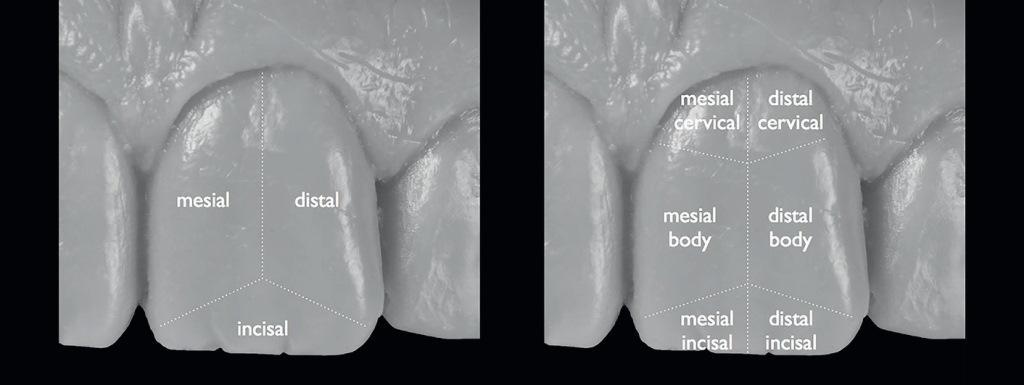
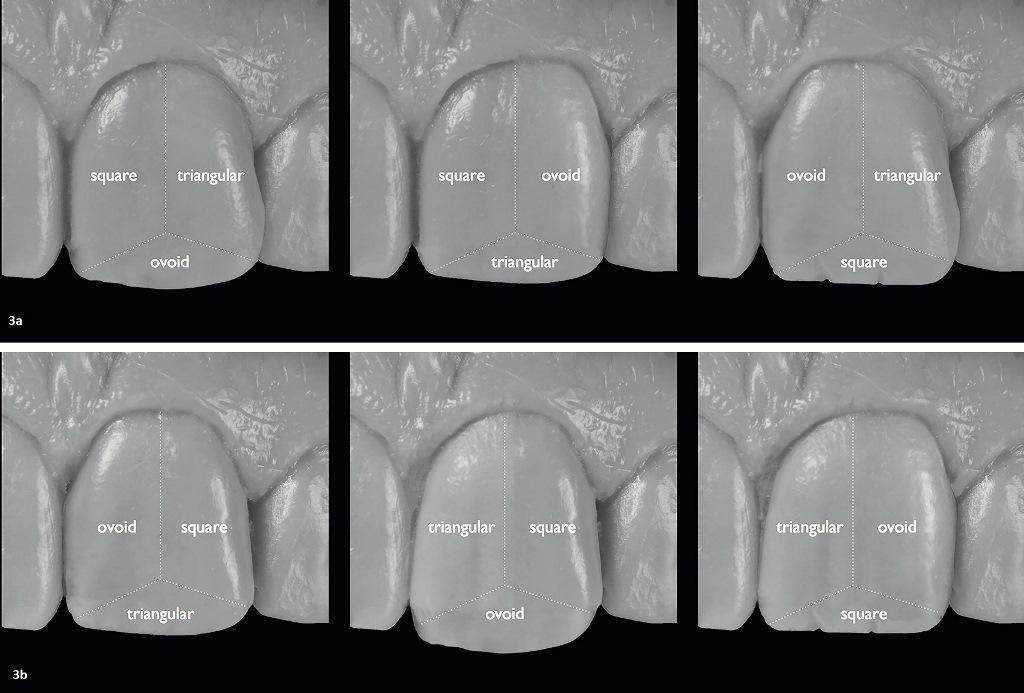
Based on the anatomical concepts and the existing configuration of the face, the approach and classification called “Dental Anatomical combinations”were used in the laboratory for the manufacture of orthopedic structures. This approach allows dentists to recreate the variable anatomy of the teeth, and not just stick to standard forms. The basic principle of this technique is to segment and combine two or even three forms of standard dental anatomy, recreating their individual shape. First, I conditionally segment the tooth surface into small sections: for example, into the central, mesial and distal segments. If necessary, these segments can be divided in half, to obtain separate mesial cervical, mesial cutting, distal cervical and distal cutting zones, as well as zones of the tooth body from the distal and mesial sides, respectively. To recreate the final shape of the tooth, full or half segments can be combined, trying to repeat the natural anatomy. The approach assumes numbering in the form 1:3, 1:2,½: 3,½: 3, which indicates which segment was used (the first digit before the colon indicates whether the segment was taken into account completely, or only half of it), as well as how many basic tooth shapes were recombinated (the second digit after the colon). The first additional class 1:3 provides for accounting for one complete segment, which is recreated by recombination of 3 main tooth shapes, as a result of which 6 different types of combinations can be obtained (photos 3a and b).
Photos 1a and b. Phase of temporary restorations: analysis of the patient’s face and reproduction of the face configuration in the form of restorations on implants.
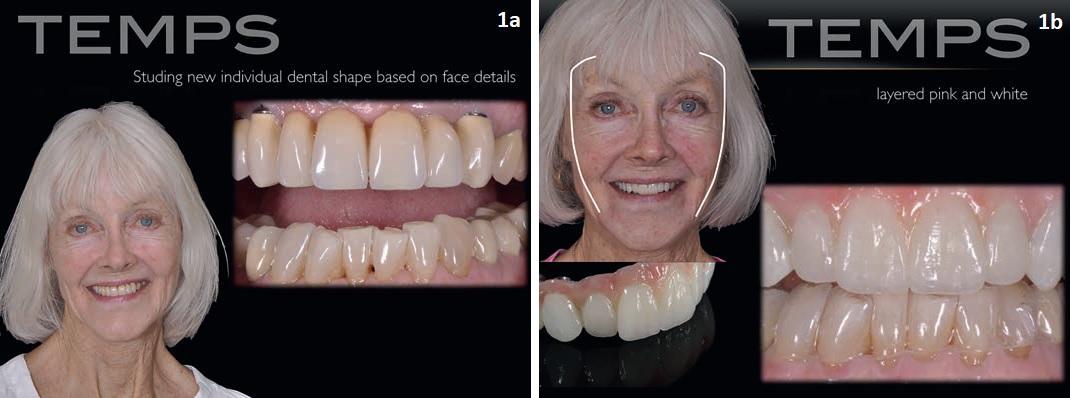
Photo 2. Segmentation of the tooth surface.
Photos 3a and b. Additional classes 1:3: combinations of three basic forms.
The second additional class, 1:2, provides for accounting for one complete segment, which is recreated by combining two main tooth shapes. This allows you to recreate 18 different tooth shapes. The third and fourth additional classes -½: 3 and½: 2, respectively, provide for accounting for half of the segments that are recreated by recombination of 3 or 2 main tooth shapes. Conditionally dividing the tooth in the vertical or oblique direction into two parts, the formed segments can be restored by varying their shape, thus giving the restoration a more dynamic appearance.
Clinical case
The analysis of the patient’s face configuration begins with the detailing of his bifrontal, bicular and bifrondibular areas (the prefix ” bi ” is used only to indicate the fact of the analysis of the face from both sides), with the design of the actual contour of the face configuration and comparing it with the future profile of the two central incisors of the upper jaw. Thus, the effect of complete individualization of the smile is achieved (photo 4a-d). With the help of veneers, which are compared on the model of the alveolar ridge, it is possible to predict changes at the level of soft tissues (photos 5-8).
Photos 4a and d. Analysis of the patient’s face. The shapes of the teeth are positioned on top of the contour of the face.

Photo 5. A model with a reproduction of the contour of soft tissues.
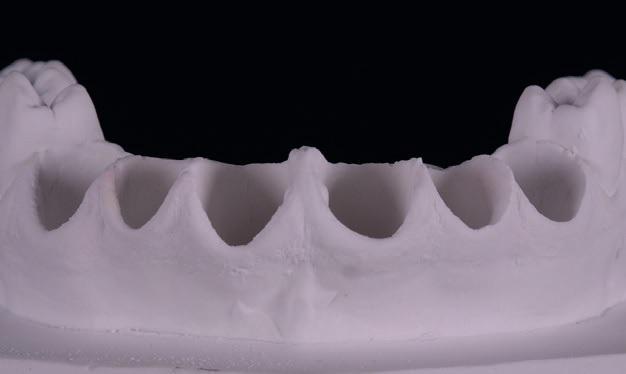
Photo 6. A model with a view of the teeth before treatment.

Photo 7. View on the refractor model.

Photos 8a and b. Modification of the contour of soft tissues.

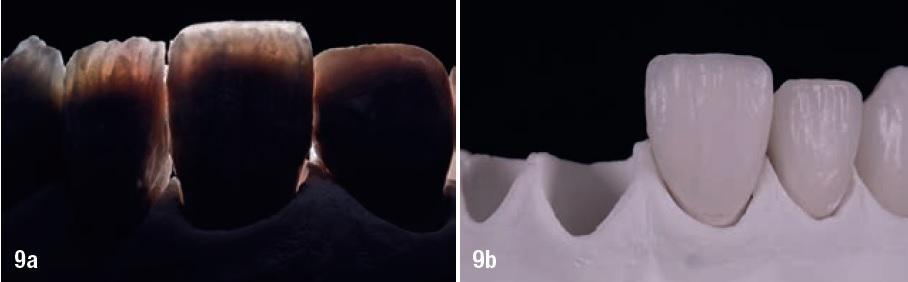
Veneers were made by the technique of layer-by-layer application of feldspar ceramics. Since the shade A1 (Creation, KLEMA Dental produkte) was chosen for the work, the shade A1 Dentin was used on the neck part of the veneer, and BD – A Dentin was used on the area from the middle part of the tooth in the direction to the cutting edge. A white transparent sample of ceramic material was compared with the surface of the tooth in the projection of the” body ” of the crown in order to assess the accuracy of the selection of the shade. In the area of the cutting edge of the veneers, several transparent ceramic masses were used, which were modified using different color shades (photos 9-13).
Photos 9a and b. Application of ceramics. a. View after the first firing.
Photos 10-11. Veneers with vertical grooves, ready for painting under a microscope.
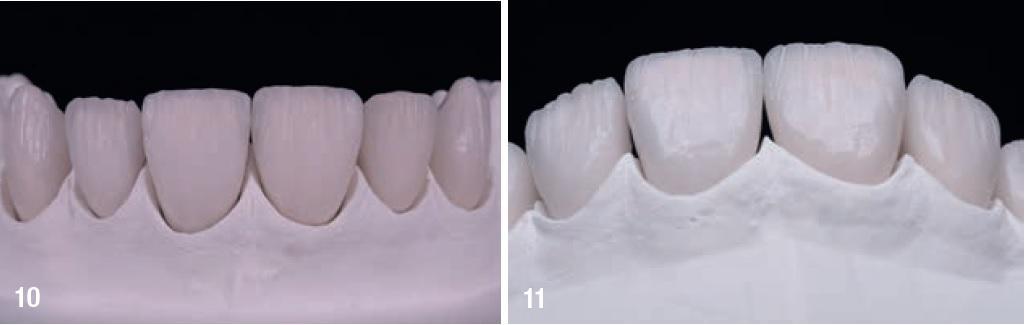
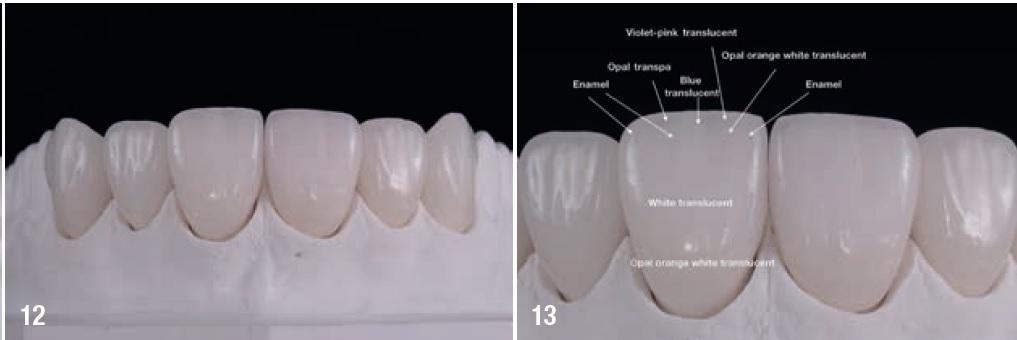
Photo 12. The final result after glazing and final processing.
Photo 13. Segmentation of the features of the superposition of ceramic masses.
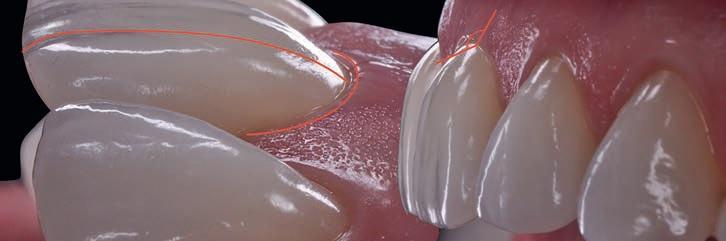
After glazing and polishing, the veneers were removed from the refractor model, and stored on a plaster master model. To assess the accuracy of the landing, an operating microscope was used. After that, another additional stage of polishing was carried out to smooth the edges of the restoration (photos 14-17). At this stage, the veneers were already fully ready for fitting in the oral cavity and further fixation. An important aspect of rehabilitation is the accuracy of the boundaries, because it is necessary to understand the difference between the visual profile and the profile angle. The visual profile implies an exact relationship between the surface contour of soft tissues and the vestibular contour of the tooth surface, in which the vestibular contour of the tooth surface should not overlap the existing contour of soft tissues. Thus, the accuracy of the visual profile depends on the soft tissues and the external contour of the tooth. The angle of the profile is associated with the accuracy of the ratio between the technical edge of the veneer and the clinically prepared ledge line. This indicator indicates the accuracy of the” fit ” of the veneers in relation to the slope of the edge of the preparation. It is logical that the angle of the veneer profile affects the visual profile of the restoration as a whole (photo 18).
Photo 14. The type of veneers after polishing.
Photo 15-17. Clear finish line and texture of veneers.
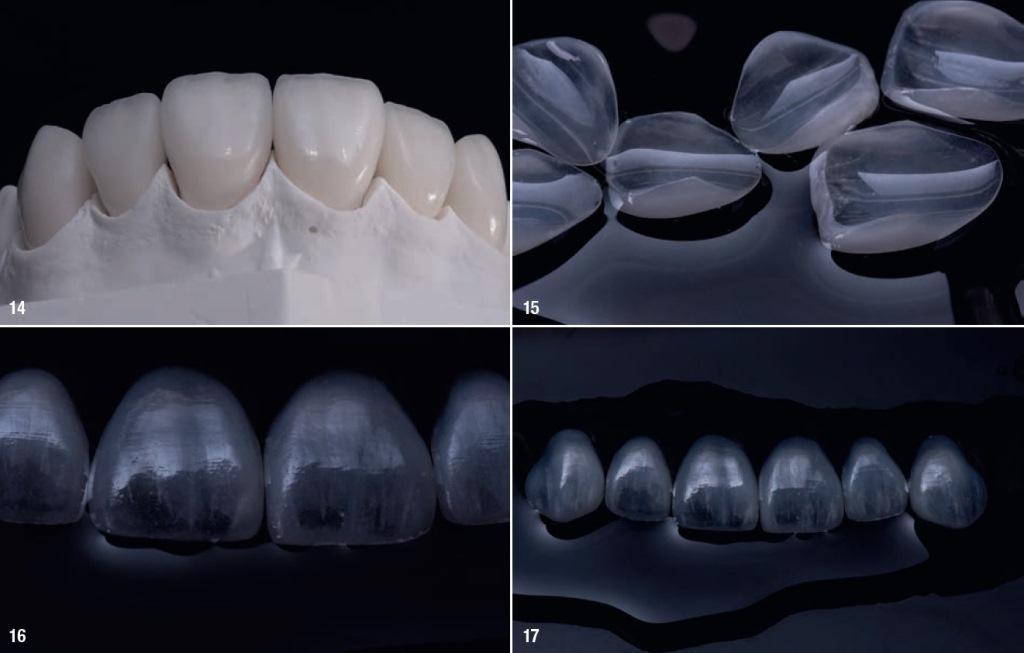
Photo 18. Visual profile (teething profile) and angular profile. Visual profile (left) of the relationship between the soft tissue area and the outer surface of the tooth. The angular profile (on the right) is the ratio between the finish line of veneers and the clinical finish line of preparation.
Conclusion
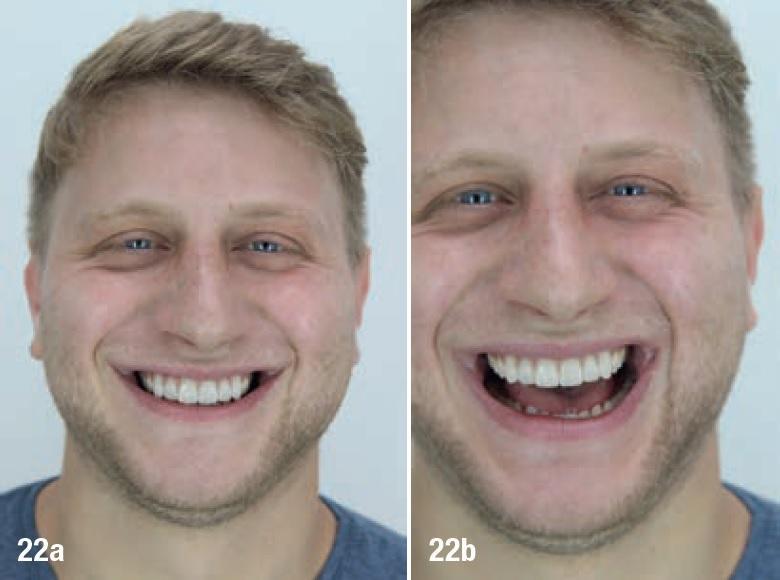
The technique described in this article provides for the implementation of the concept of planning an individual tooth shape based on the profile of the patient’s face. Understanding all the possibilities of anatomical configurations, by combining variations of individual segments of the teeth and the cutting edge, it is possible to recreate the individual morphology of the external profile of the tooth, abandoning the standard variants of such. From a technical point of view, it is extremely important to determine the approach to planning and designing various contours of a smile that allow you to simulate the appearance of natural teeth as much as possible (photos 19-22). By combining digital and analog protocols, the dentist and the technician can develop a joint constructive way to individualize the shape of the teeth, based on the configuration of the patient’s face profile, thus ensuring the maximum predicted outcome of aesthetic rehabilitation.
Photo 19. Photo of the patient’s face before treatment.

Photo 20. The type of teeth before treatment.

Photos 21a and c. Type of veneers without preparation: from 13 to 23 teeth.

Photos 22a and b. Individualization of a smile. The harmonic ratio of the shape of the teeth with the external configuration of the face.